

The report was co-authored by Duff & Phelps and Norton Rose Fulbright.
Introduction
The behavioral healthcare industry continues to grow, with a
significant imbalance between patient demand and patient access to
care. In 2016, an estimated 44.7 million adults had a mental
illness such as depression, anxiety or schizophrenia, but only 43%
received proper treatment,1 leaving more than 25 million
Americans without adequate care. Similarly, over 19 million adults
have an addiction problem, but only 16% are receiving proper
treatment.2 Behavioral health providers remain in high
demand across the country. As of 2015, approximately 55% of the
nation's 3,100 counties do not have any practicing
psychiatrists, psychologists or social workers.3
Healthcare providers and investors are responding to the imbalance
by aggressively growing behavioral health practices organically or
via acquisition to meet the high demand. As providers grow, they
are inevitably faced with the prospect of expanding their practices
across state lines. This article addresses the implications of a
multi-state expansion strategy from a variety of viewpoints. It
will discuss the value creation, regulatory and compliance
challenges and other operating considerations of a multi-state
behavioral healthcare practice.
Creating Value Through Multi-State Strategies
According to IBISWorld, an estimated 77% of the 10,000 companies
operating substance abuse treatment clinics have a single location,
and 57% of all clinics have fewer than 20 employees.4 As
patient demand for care and the availability of governmental and
commercial reimbursement continue to expand the industry,
consolidation will reduce the number of small providers as large
platform investments create regional and national practices. The
advantages of multi-state practices compared to small, single-state
providers will be quite notable. Multi-state practices have
significant competitive advantages over small providers, including
but not limit to, the stability of their cash flows and the
opportunity to profitability expand those cash flows in the
future.
Diversified Payor Base
While all healthcare practices face reimbursement risk, multi-state
practices benefit from a diversified payor base that creates a more
stable cash flow stream. Given the implementation and increasing
enforcement of federal mental health parity laws and regulations
across states, most behavioral healthcare providers, like all other
healthcare providers, are now beholden to third-party payor
reimbursement rates from private insurance or state-sponsored
programs. Although contracting with governmental and commercial
payors in multiple states comes with its challenges, multi-state
practices are less impacted by changes in reimbursement policies by
any one state, territory or payor, because of their diversified
reimbursement base. This makes their overall annual cash flows more
stable. Diversified reimbursement from a variety of payors,
especially diversified Medicaid state reimbursement, lowers the
financial risk profile of a multi-state behavioral health practice
and therefore creates value for the owners of the practice. The
payor universe for mental health and substance abuse centers is
dominated by Medicaid, which accounted for approximately 33% of
2017 industry revenue of $16.3 billion.5 According to
the Medicaid and CHIP Payment and Access Commission (MACPAC),
Medicaid payments for inpatient services vary considerably across
states, ranging from 49% to 169% of the national
average.6 Similar to a diversified stock portfolio where
decreases in value of one position are often offset by increases in
value of another, any impact of Medicaid reimbursement variability
or changes thereto is likely less severe for practices with a
diversified state payor mix. In 2018, Medicaid rates are expected
to rise in 44 states for at least one provider type, such as
inpatient and outpatient hospitals, primary care physicians,
specialists, dentists or nursing homes.7 However, only
17 states plan to increase inpatient hospital rates this year,
while 33 states plan to cut or keep rates the
same.8
The underlying determinates of Medicaid reimbursement are complex
and oftentimes political, with each state formulating its own plan
and scope of services to be covered. This complexity makes it
essential to diversify one's payor base and gives behavioral
healthcare providers operating in multiple states a significant
advantage because the risk of Medicaid reimbursement changes is
unlikely to occur evenly across state programs.
Economies of Scale
Further value is created by multi-state practices from economies of
scale. These size advantages can lead to improved profit margins
and return on growth investments. As practices seek to gain larger
market share appropriately structured marketing programs are
crucial to increasing brand awareness, referrals and ultimately
patient flow. National and regional marketing efforts leverage
programs across larger patient populations, improving the cost
structure as more locations are added and the marginal cost of
marketing decreases. For example, AAC Holdings (AAC), a provider of
inpatient and outpatient substance abuse treatment, has achieved
success by developing a national brand, American Addiction Centers,
through investment in its facilities and expertise in its national
marketing program. The centralization of one national or regional
marketing effort resulted in significant inbound volume from
potential clients.9 Furthermore, a multi-state
geographic strategy and marketing plan covering a large region can
capture a greater number of referrals, driving additional revenues
to a practice.
Recruitment of physicians and other behavioral health
professionals is crucial to the success of any healthcare practice.
Multi-state practices have the benefit of notoriety and resources
to enable the recruitment of top candidates. The issues of
recruitment are compounded for single-state practices located in
smaller or rural markets. Physicians are typically trained in large
metropolitan areas and tend to stay in those areas following
their training. Research shows that fewer than 3% of newly trained
physicians prefer a community of 25,000 residents or less, while
59% prefer a community of 100,000 or more people.10
Moreover, practices with multiple offices in close proximity can
more effectively manage workflow for behavioral health
professionals and mitigate staffing imbalances.
Advantages in marketing and physician recruitment are two examples
that demonstrate how multi-state practices leverage economies of
scale. Other economies of scale relate to general back-office
support and technology services that reduce practice costs. For
example, AAC maintains a 24/7 call center at its corporate
headquarters that conducts benefits verification and handles
communication with insurance companies for all its facilities. In
addition, AAC centralizes functions such as accounting, billing and
collections allowing its facilities to focus solely on providing
clinical care.11 Similarly, the use and implementation
of electronic medical records (EMRs) in behavioral health has
improved information capture, reporting and data aggregation.
Technology enables behavioral health organizations to operate
seamlessly across multiple geographies. A multi-state strategy also
allows a practice to further scale its billing and collections
efforts. Accounts receivable management for behavioral health
practices is less complex than medical/surgical hospital providers
because behavioral healthcare facilities have fewer billing codes
and generally are paid on a per diem basis. Therefore, as
behavioral health practices grow, billing and collections scale can
provide operating leverage and margin
improvement.12
Telehealth Services
The rapid growth of the telehealth industry over the past several
years and its use in behavioral health settings provides
opportunities to further improve operations for multi-state
practices. Telehealth is generally defined as the use of electronic
information and telecommunications technologies, such as
videoconferencing and electronic messaging, to provide healthcare.
The telehealth industry, which is expected to grow at nearly 10%
over the next 5 years,13 is leveraging advances in
communication and medical technologies, such as wearable devices,
digitized medical scans and more efficient treatment delivery.
Telehealth is increasingly being used to deliver behavioral
health services. With access to telehealth tools, patients and
physicians in different locations can interact via live
(synchronous) healthcare sessions, enabling behavioral health
practices to expand coverage and provide services to patients in
underserved areas. According to research studies, telehealth
services can even prove more effective than in-person visits due to
the comfort and ease of meetings with healthcare
providers.14 Telehealth enables providers of behavioral
health services to potentially expand their service area across
state lines, without the time and expense of burdensome state
facility licensure requirements that may be required to build a
brick and mortar facility. Telehealth allows providers to serve an
increased patient population while delivering cost savings,
specifically by reducing patient no-shows, cancellations and the
costs associated with establishing and running multiple brick and
mortar facilities.15
Regulatory Considerations in Implementing a Multi-State Strategy
As discussed above, there are many advantages to a multi-state
strategy in the provision of behavioral health services. However,
key regulatory regimes applicable to behavioral health vary on a
state-by-state basis and need to be considered and complied with in
a manner that is effective and practical at an organizational level
when executing a multi-state strategy.
Professional Licensure and Telehealth
Physician and other behavioral health professional licensure
requirements vary by state and can present issues for providers
wishing to administer behavioral health services across state
lines. There are also inconsistencies among states' laws and
regulations regarding the practice of medicine. Thus, a physician
engaged in telehealth services across state lines may be
responsible for complying with multiple sets of licensure laws and
medical practice regulations. Physicians who want to practice
telemedicine in multiple states may be eligible to apply for a
license through the Interstate Medical Licensure Compact (IMLC),
which allows licensed physicians to practice medicine across state
lines if they meet certain eligibility requirements and are located
in one of the 22 IMLC member states. However, states also have
varying requirements applicable to telehealth communication
modalities (video, audio, etc.), e-prescriptions, the establishment
of patient-provider relationship, and locations where the services
can be provided (e.g., the patient's home versus an outpatient
setting where the patient resides).
State and Federal Privacy Regimes
State and federal privacy laws and regulations contain varying
protections for patients' behavioral health records. On the
federal side, these laws include the Health Insurance Portability
and Accountability Act of 1996 and its implementing regulations
(collectively, HIPAA), and the Confidentiality of Alcohol and Drug
Abuse Patient Records regulations (42 CFR Part 2) promulgated by
SAMHSA, often referred to as the SAMHSA Regulations. The SAMHSA
Regulations are applicable to any patient records maintained by an
alcohol and drug treatment program that receives federal funding
(e.g., Medicare, Medicaid or a grant of tax-exempt status) and are
much more stringent than HIPAA, providing few avenues for sharing
patient information (e.g., between providers) without patient
consent for each disclosure. The SAMHSA Regulations were amended
effective March 21, 2017, with the intent of facilitating
integration of care and incorporating new healthcare delivery
models while also protecting the privacy of patients seeking
treatment for substance use disorders. There is a divergence of
viewpoints between those who want more data sharing to improve care
coordination and those who are concerned about the negative
consequences (e.g., employment discrimination and potential
prosecution, etc.) of the release of sensitive substance abuse
information, as to whether the SAMHSA Regulations, as amended, go
too far or not far enough. Regardless, the disclosure requirements
of the SAMHSA Regulations continue to be more stringent than and
not aligned with HIPAA, and substance use disorder programs that
receive federal reimbursement are required to comply with both
federal regulatory regimes.
In addition, all states and the District of Columbia have enacted
laws to protect their citizens' health records. The challenge
from a compliance perspective is the many inconsistencies between
federal and state privacy laws. Some state privacy laws directly
conflict with the standards set forth in HIPAA. In these instances,
the more stringent law will apply, which is often the case with
state privacy laws applicable to behavioral health. Thus, a
multi-state behavioral health organization would need to enact a
privacy compliance program that incorporates both HIPAA and the
most stringent state law requirements, and if it operates any
federally funded substance use disorder programs, the SAMHSA
Regulations as well.
Corporate Practice of Medicine
The corporate practice of medicine (CPOM) doctrine has its roots in
seeking to prohibit non-physicians from interfering with a
physician's professional judgment by barring legal entities not
owned or controlled by physicians from employing physicians to
practice medicine and charging for those professional services.
However, the actual restrictions and permitted exceptions vary
significantly by state, and some states do not have a CPOM
restriction at all. Further, depending on the state, the doctrine
often extends beyond physicians to other licensed professionals
such as psychologists and licensed social workers. In states with
CPOM restrictions, the professional practices must generally be
owned by physicians or other licensed professionals only, and
ownership by non-licensed individuals or corporate entities is not
permitted.
A multi-state behavioral health provider must examine whether each
state in which it plans to operate has CPOM restrictions, and, if
so, how the operation of its business in that state should be
structured to comply with the requirements. For example, many CPOM
states will allow a business entity that is not owned by licensed
professionals to provide non-clinical business management and
administrative services (e.g., financial management, office space,
clerical staff, billing and collections) to the licensed,
professional-owned entity that employs the behavioral health
providers. However, states vary in their requirements related to
permissible financial arrangements between the professional entity
and the management services organization. Further, arrangements
between the management services organization and the professional
entity must be structured to ensure that non-licensed professionals
cannot influence the professional judgment of the providers
employed by the professional services entity.
Facility and Program Licensure
Another area where pertinent regulations vary on a state-by-state
basis relates to the licensure to establish, significantly modify
or wind-down behavioral health facilities and programs. For
example, New York requires a wide range of behavioral health
facilities and programs to obtain a license from the New York State
Office of Mental Health, including psychiatric emergency programs,
residential treatment programs, psychiatric units in general
hospitals, free-standing psychiatric hospitals and outpatient
programs.
As another example, California allows voluntary facility
certification for day treatment, outpatient and nonresidential
detoxification facilities that meet or exceed specific service
quality and program standards. On the other hand, licensure is
required to operate community residential treatment systems and
skilled nursing facilities which treat patients with acute or
chronic psychiatric conditions. Licensure is also required to
operate non-medical residential facilities in California that
provide care and supervision to people who are unable to live by
themselves but who do not need full-time nursing care, and who can
benefit from detoxification programs, group and individual
counseling and recovery treatment planning offered at the
facilities.
The licensure requirements are intended to allow the state to establish standards for the quality and adequacy of behavioral health facilities and programs in the state, and to enable the applicable state agency to conduct surveys, inspections and investigations of facilities and programs, including their books and records. Non-compliance by licensed facilities and programs may result in a requirement to submit a plan of corrective action, fines or loss of licensure.
States can vary widely with respect to types of licenses
required, the process and timing to obtain the licenses and the
requirements for maintaining them. Licensure applications and
renewals often involve substantial disclosures regarding the
program, community needs, staffing, finances, facilities, ownership
and various other matters, as well as inspections by and meetings
with the state regulators. Thus, a multi-state operator of
behavioral health facilities and programs needs to dedicate
adequate time and resources to ensure compliance with individual
state requirements.
Reimbursement
Governmental and commercial reimbursement rates for behavioral
health services can vary significantly across states. For example,
see the discussion regarding Medicaid reimbursement in Section 2
above. In addition, multi-state operators often need to negotiate
separate governmental and commercial contracts for each state in
which they operate. Negotiating and administering these contracts
requires a considerable level of resources.
Moreover, a multi-state operator must engage in extensive financial
planning to account for the variability in rates across states.
While diversity in rate regimes and reimbursement schedules may
provide some revenue stability, complex planning and patient and
payor analytics may be necessary to execute a profitable
multi-state strategy.
Growth Considerations for Multi-State Practices
While there is inherent value in operating as a multi-state
practice, the challenges to effectively grow and scale into a
larger operation, as outlined in Section 3, must be considered. One
of the first topics to consider is a contiguous state approach
versus a noncontiguous state approach. A contiguous state approach
will provide geographic economies of scale such as advertising,
patient referrals and physician recruitment. Furthermore, a
contiguous strategy may provide the opportunity to develop more
vertically integrated care delivery models where behavioral health
practices integrate with primary care and other specialties.
Research has shown that integrated care improves patient
outcomes, reduces reimbursement issues, increases employee
productivity, boosts employee satisfaction and decreases
costs.16 Practices that operate across primary care and
behavioral care are able to treat patients within their practice
more efficiently by providing comprehensive care services, likely
improving outcomes for the patient and increasing revenue
opportunities. According to research from the University of
Michigan, best practices in integrated care require creating a
culture of collaboration within the organization, engaging
employees in orientation or training programs, and using a
cooperative approach to foster a system of "warm
hand-offs" between physicians to improve patient
care.17
However, the contiguous state approach may not lend itself to
targeting the largest potential customer base. Behavioral health
demand is spread across the country, with mental health issues
varying by state and region. For example, in 2017, an estimated
12.5% of California's population 12 years of age and older
experienced substance dependence or abuse, with no other state in
the Western region experiencing more than 3%. Similarly, in 2017,
Texas, Minnesota, Florida and North Carolina all experienced levels
above 3% with no contiguous state above the 3% threshold.18 With
concentration spread so unevenly across the country, behavioral
health practices may look to high-demand regions for growth,
requiring noncontiguous state expansion strategies.
Private equity firms looking to invest in behavioral health
practices can be helpful in developing and implementing a
multi-state strategy. Financial sponsors focus on adding value to
investments through improving margins and driving growth via
organic expansion or acquisitions. Private equity backed
acquisition roll-ups of smaller providers may be able to drive
significant economies of scale, resulting in both clinical and
administrative standardization. In other areas of the healthcare
market, such standardization has resulted in improved health
outcomes and decreased costs.20 Multi-state practices will likely
receive more attractive valuations given the potential for growth
and expansion, whether completed organically or via acquisition.
Behavioral health practices with large multi-state operations and a
demonstrated track record of successful entry into new geographies
are likely to command premium valuations.
2017 M&A Activity
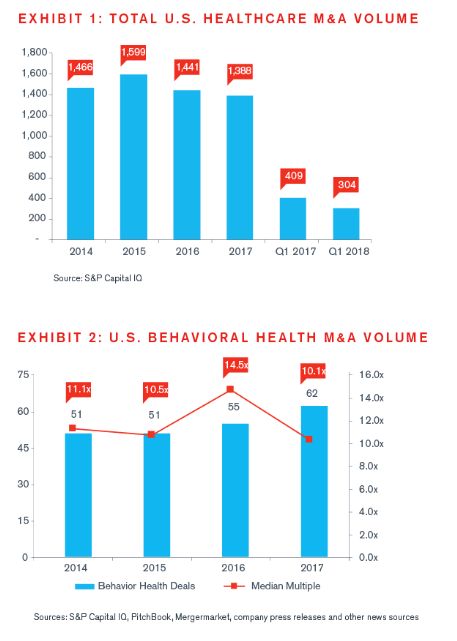
In 2017, according to S&P Capital IQ, 62 behavioral health transactions were announced, which shows a steady increase from the 55 transactions announced in 2016, continuing a robust trend of acquisition activity in the behavioral health sector. Behavioral health transaction multiples have remained strong, with a 2017 median EBITDA multiple of 10.1x, falling in line with recent multiples.
Given the continuing imbalance between patient demand and patient access to care, provider market fragmentation, and continued expansion of reimbursement based on the continued implementation and enforcement of federal mental health parity laws, we expect to see continued growth in deal volume in the area of behavioral health in the years to come.

Footnotes
1 Substance Abuse and Mental Health Services
Administration. (2017). Key substance use and mental health
indicators in the United States: Results from the 2016 National
Survey on Drug Use and Health (HHS Publication No. SMA 17-5044,
NSDUH Series H-52). Rockville, MD: Center for Behavioral Health
Statistics and Quality, Substance Abuse and Mental Health Services
Administration. Retrieved from https://www.samhsa.gov/data/
2 Kaiser Family Foundation, "Medicaid's Role in
Behavioral Health," May 5, 2017,
https://www.kff.org/infographic/medicaids-role-in-behavioral-health/
3 Rene Quashie, "The Boom in Telemental Health,"
TechHealth Perspectives, August 2015, https://www.techhealthperspectives.com/2015/08/24/the-boom-in-telemental-health/
4 IBISWorld, Mental Health & Substance Abuse Centers in
the US, March 2017
5 Ibid
6 "Medicaid Hospital Payment: A Comparison Across States
and to Medicare," MACPAC, April 2017,
https://www.macpac.gov/publication/medicaid-hospital-payment-a-comparison-across-states-and-to-medicare/
7 Virgil Dickson, "Medicaid Rates in 44 States to Rise in
Fiscal 2018," Modern Healthcare, October 20, 2017,
http://www.modernhealthcare.com/article/20171020/NEWS/171029989
8 Ibid
9 AAC Holdings Inc. 2017 10-K
10 Merritt Hawkins White Paper Series, "Rural Physician
Recruiting Challenges and Solutions," 2016
11 Ibid
12 Acadia Healthcare Inc. 2017 10-K
13 IBISWorld, Telehealth Services in the US, May 2017
14 Meredith Lawrence, "The Benefits of Telemental Health
to Patient and Provider," January 2015,
http://theworkspacetoday.com/2015/01/20/benefits-telemental-health-patient-provider-qa-dr-marlene-maheu/
15 Zereana Jess-Huff, "How Telehealth Can Transform
Behavioral Health Care," April 2016,
http://www.benefitspro.com/2016/04/26/how-telehealth-can-transform-behavioral-health-car?t=wellness&page=2&slreturn=1518137153;
16 University of Michigan, "Primary Care and Behavioral
Health Workforce Integration: Barriers and Best Practices",
February 2017, http://www.behavioralhealthworkforce.org/wp-content/uploads/2017/02/FA2P3_Team-based-Care-Case-Studies_Full-Report.pdf
17 Ibid
18 IBISWorld, Mental Health & Substance Abuse Centers in
the US, March 2017
The content of this article is intended to provide a general guide to the subject matter. Specialist advice should be sought about your specific circumstances.

